|
Histopathology and Surgical Pathology
A main and important routing work in our Department is histopathology (needle biopsy pathology) and surgical pathology (surgical sample pathology). As a pathologist, not only for histopathology, also for surgical pathology, we must know our own field comprehensively, but we must also have a broad background in clinical medicine, understand the clinician’s needs, respond to them accordingly and often we should discuss with them for diagnosis and treatment aims. We must be in a position to advise the clinician about the biopsy or the excised material we receive. Reporting whether a lesion is benign or malignant is not enough, we must be able to tell the surgeon the extent of the disease, the grade of malignancy, the adequacy of the excision, and other relevant information, to comment on whether additional therapy may be necessary and give information on the prognosis of disease. Various samples for research for pathologic diagnosis are also welcome in our Department.
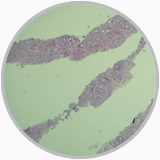
A punctural biopsy sample from a patient of prostat adenocarcinoma |
Histology shows prostat adenocarcinoma, Gleason score 6 |

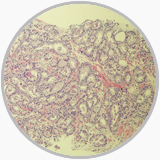
A gastric sample from a patient underwent a gastrectomy |
Histology shows middle deffenrentiation adenocarcinoma |
Special Staining Technique in Pathology
HE staining is a basic staining technique in surgical pathology, and many special staining techniques are now stile valuable for diagnostic aims. The most commonly used techniques in our Department are ① Congo red staining is regarded as the most reliable and practical technique for detecting amyloid material; ② Periodic acid-Schiff (PAS) stain is extremely useful to detect glycogen and neutral mucosubstances, to outline basement membranes and to demonstrate most types of fungi and parasites; ③ Reticulum stains may point reticular fibers and basement membrane material. The silver-based reticulum stains are useful in tumor pathology in distinguishing epithelial from non-epithelial neoplasms, various mesenchymal neoplasms from each other and in situ from invasive carcinoma. ④ A combination of Alcian blue and PAS may demonstrate various mucosubstances such as neutral, slightly acidic and highly acidic mucus. In addition we use also Trichrome stains and stains for neutral lipids if it necessary.
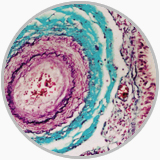
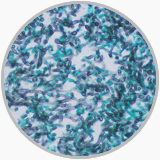
A tricolor staining shows an artery and a vein |
A silver staining shows Fungi |
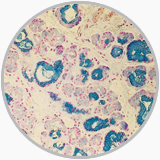
A ferrum staining in a liver biopsy |
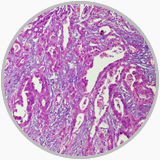
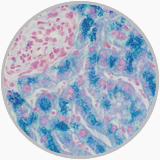
Alcian blue staining in a gastric biopsy |
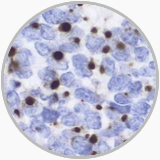
Immunohistochemistry (IHC) Technique
The utility and improvement of IHC Technique has strongly revolutionized the pathology, not only because of its highly sensitivity and specificity, applicability to routinely processed material, but also the feasibility of an accurate correlation with the traditional morphologic parameters. It is sometimes critical in helping a pathologist for diagnosis and differentiation diagnosis. Important is that for any ambiguous case it be carefully observed at HE staining following key differentiation diagnosis and antibody selection. Additionally, it is necessary to establish a standardized IHC staining protocol including suitable tissue fixing, efficient antigen retrieval, pertinent pH value, a positive and negative control and a correct judgment of IHC results.
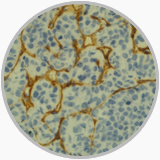
CD34 positivity showed in sinusoids in hepatocellular carcinoma |
A paranuclear dot-like staining of CD99 in a pancreatic solid pseudopapillary tumor |
A special dot-like positivity of CK20 in a Mekel carcinoma |
Immunohistochemistry shows no staining of 34BE12 in prostat gland carcinoma but reactivity in normal glands and ductules |
|
